
The incisura fibularis is a key anatomical feature of the distal tibia that plays a central role in the stability, biomechanics, and injury patterns of the ankle mortise, with growing relevance to podiatric practice and contemporary imaging‑guided management of ankle trauma. This essay will outline its anatomy, morphological variability, radiological assessment, and clinical significance, particularly in relation to syndesmotic injury, posterior malleolar fractures, and recurrent lateral ankle sprain.
Anatomy and basic function
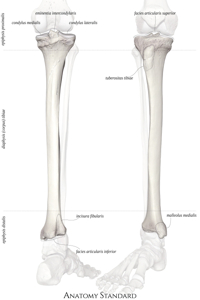
The incisura fibularis (fibular notch) is a triangular depression on the posterolateral aspect of the distal tibia that receives the distal fibula. Together with the distal fibula and the distal tibiofibular ligaments, it forms the distal tibiofibular syndesmosis, which is crucial for maintaining the congruence of the ankle mortise around the talus.
Bony congruity between the medial surface of the fibula and the walls of the incisura provides an important component of syndesmotic stability, complementing the anterior inferior tibiofibular ligament, posterior inferior tibiofibular ligament, interosseous ligament, and transverse tibiofibular ligament. The geometry of the notch constrains fibular translation and rotation, thereby influencing talar position under load and the distribution of forces across the tibiotalar joint.
Morphological variability
Morphometry studies have demonstrated substantial anatomical variability in incisura depth, height, width, and orientation, with some evidence of gender‑related differences. Descriptions commonly distinguish shallow versus deep notches and note variations in version (anteverted, neutral, retroverted) and in how well the fibula “engages” within the notch.
Three broad distal tibial surface shapes have been described on CT and 3D models: a “C‑shaped” configuration producing a crescent‑shaped syndesmosis, a “1‑shaped” configuration with a relatively shallow incisura, and a “G‑shaped” configuration with a deeper notch and more prominent anterior or posterior tibial tubercles. These morphotypes appear to correlate with different patterns of fibular seating, posterior malleolar fracture morphology, and propensity to ligamentous versus bony injury.
Radiological assessment
Radiologically, the incisura fibularis has become a central landmark for intra‑ and postoperative assessment of syndesmotic reduction following ankle fracture or high‑ankle sprain. On mortise view radiographs, the lateral border of the talus normally aligns closely with a line projected from the proximal incisura down to the tibial plafond, reflecting mortise congruence.
In ankles without fracture, dislocation, or syndesmotic disruption, the alignment between the incisura and the lateral talar border is typically within 1 mm; a deviation of 1 mm or more has been proposed to indicate mortise incongruence and possible syndesmotic instability or talar shift. CT‑based measurements of incisura depth, rotation, width, and fibular engagement have also been used to validate syndesmotic reduction, with small side‑to‑side differences in depth and rotation when the syndesmosis is anatomically restored.
Relationship to injury patterns
A growing body of work links incisura morphology to specific ankle injury patterns. A shallow, retroverted, or “disengaged” incisura appears more frequently in patients with ligamentous syndesmotic injury and recurrent lateral ankle sprain, suggesting reduced bony constraint and greater reliance on soft tissues for stability. In such individuals, inversion injuries may preferentially overload the anterior talofibular ligament and syndesmotic structures rather than resulting in straightforward malleolar fractures.
Conversely, deeper, more constraining notches may predispose to particular posterior malleolar fracture configurations when axial load and rotational forces are transmitted through the tibiofibular complex. A recent retrospective CT‑based study of posterior malleolus fractures reported significant associations between incisura depth, version, width, fibular engagement, and the pattern of posterior malleolar involvement, including statistically significant relationships between incisura width and fracture type and between fibular engagement and fracture pattern.
Surgical and intraoperative relevance
Intraoperatively, the incisura fibularis is used as a bony reference for anatomic reduction of the distal fibula, particularly in syndesmotic fixation after malleolar fractures. Malreduction, especially excessive external rotation or lateral translation of the fibula relative to the incisura, is a recognised cause of poor outcomes, and its prevention depends on understanding the patient‑specific notch anatomy.
Techniques that allow direct visualization and manipulation of the incisura—such as posterior approaches that expose the distal tibial plafond and tibiofibular junction—permit more accurate restoration of the fibula into the notch before definitive fixation. For isolated distal tibiofibular arthritis or chronic syndesmotic instability, fusion procedures rely on preparing the joint surfaces within the incisura–fibula interface to achieve solid arthrodesis while preserving overall ankle alignment and mortise geometry.
Implications for podiatric practice
For podiatrists and foot and ankle clinicians, awareness of incisura fibularis morphology has several practical implications. First, when interpreting ankle radiographs or cross‑sectional imaging after sprain or fracture, recognising a congenitally shallow or retroverted notch can help explain recurrent instability or atypical injury patterns and inform discussions about prognosis. Second, in patients with chronic symptoms after “adequately treated” ankle fractures, subtle syndesmotic malreduction relative to the incisura may underlie persistent pain, dysfunction, or early degenerative change.
Finally, as CT‑based classification systems and morphometric analyses become more integrated into surgical planning, podiatric practitioners collaborating in multidisciplinary teams need a clear conceptual model of how the incisura contributes to distal tibiofibular stability and to posterior malleolar fracture morphology. This knowledge supports more nuanced rehabilitation strategies, targeted protection of at‑risk ankles, and more accurate communication of radiological findings and surgical objectives in the management of complex ankle injuries.