
The Lunge Test provides a reliable, weight-bearing measure of ankle dorsiflexion range of motion, essential for assessing functional mobility in clinical practice. Commonly known as the Weight-Bearing Lunge Test (WBLT) or Knee-to-Wall Test, it simulates real-world movements like walking or squatting. This essay explores its procedure, reliability, clinical applications, normative values, and limitations in podiatry and rehabilitation.
Test Procedure
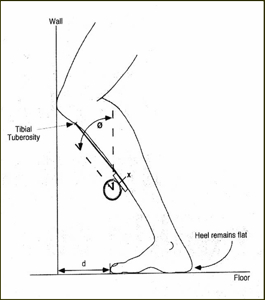
Perform the Lunge Test with the patient facing a wall, feet parallel and hip-width apart. Position the test foot 10 cm from the wall initially, then lunge forward by flexing the knee toward the wall while keeping the heel flat on the floor and the knee aligned over the foot. Advance or retract the foot until the knee just touches the wall at maximal dorsiflexion without heel lift.
Measure maximum toe-to-wall distance using a tape measure or ruler placed along the floor from the wall to the hallux (big toe). Alternatively, use an inclinometer on the tibia to record the angle from vertical, typically 35-38 degrees for normal function. Repeat three times per leg, averaging results, with shoes and orthotics if relevant to daily use.
This line drawing illustrates proper lunge positioning, highlighting heel contact, knee-to-wall alignment, and toe-to-wall measurement (d).
Reliability and Validity
The WBLT demonstrates high intra-rater, inter-rater, and test-retest reliability, with intraclass correlation coefficients (ICCs) exceeding 0.92 across studies. Powden et al. (2015) found no significant differences in reliability between tape measure, inclinometer, or plumb line methods, confirming its consistency for talocrural dorsiflexion.
Concurrent validity is strong against non-weight-bearing goniometry (r=0.80-0.95), though it better captures functional restrictions from soft tissue or joint stiffness. In stroke patients, it correlates moderately with gait velocity (r=0.605), Timed Up and Go (r=-0.598), and Functional Ambulation Category (r=0.380), validating its gait relevance.
Normative Values
Normal toe-to-wall distance averages 12.5 cm (5 inches) or more, equivalent to one hand-width, indicating adequate dorsiflexion for activities like running. Tibial angle norms range 35-38 degrees; below 35 degrees signals restriction, increasing injury risk in athletes.
Values vary by population: athletes require >10 cm for lower extremity injury prevention, while <9-10 cm predicts musculoskeletal issues in sports like Australian football. In podiatry, restrictions often stem from gastrocnemius/soleus tightness or talocrural joint limitations.
Clinical Applications
Podiatrists use the Lunge Test to evaluate ankle dorsiflexion deficits contributing to conditions like plantar fasciitis, Achilles tendinopathy, or patellofemoral pain. Reduced range correlates with altered gait mechanics, excessive pronation, and forefoot overload, guiding orthotic prescriptions or footwear modifications.
In rehabilitation, it tracks progress post-injury or intervention; Botulinum Toxin for spastic equinus in stroke improved median ALT from 20 mm to 21 mm (p<0.02) alongside better Timed Up and Go scores. Anterior knee pain or “pinching” during testing suggests joint capsule restrictions amenable to mobilizations, while posterior calf tightness benefits from stretching or foam rolling.
For golfers or runners—common podiatry patients—deficits heighten injury risk; serial testing informs biomechanics interventions.
This image shows the wall test in action, emphasizing knee drive and heel grounding for accurate assessment.
Biomechanical Insights
Ankle dorsiflexion, primarily talocrural motion, requires 10-15 degrees for normal gait but up to 30 degrees in squatting or lunging. The WBLT measures composite stiffness including gastrocnemius, soleus, and joint arthrokinematics under load, unlike supine tests that ignore muscle tone.
Restrictions elevate tibial shear forces, promote compensatory subtalar eversion, and strain the kinetic chain, explaining links to lower limb injuries. In evidence-based podiatry, it differentiates neural (spasticity) from musculoskeletal limits, prioritizing targeted therapies.
Limitations and Considerations
While reliable, the test assumes symmetrical foot placement and may overestimate dorsiflexion in pronated feet or underestimate in cavus deformities. It conflates talocrural and subtalar contributions, so adjunct tests like lunge with knee extended (gastrocnemius bias) enhance specificity.
Ceiling effects occur in hypermobile individuals, and floor effects in severe restrictions; inclinometry mitigates this. Perform bilaterally for asymmetry detection, and standardize with shoes/orthoses to reflect functional ROM. Patient factors like pain or balance impair performance, necessitating supervision.
Interventions Based on Results
Restricted results (<10 cm) prompt a tiered approach: soft tissue mobilization (calf stretching, foam rolling) for muscular limits, or high-velocity joint mobilizations (e.g., posterior talar glides) for capsular restrictions. Orthotics with rearfoot posting restore alignment, while minimalist footwear trains dorsiflexion in mild cases.
Reassess weekly; gains of 2-3 cm correlate with functional improvements. In pseudoscience-heavy foot care markets, emphasize WBLT’s evidence over anecdotal “barefoot resets” [user interests].
Evidence in Podiatry Practice
Studies affirm its predictive validity: Australian footballers with lunge deficits faced higher injury rates, underscoring screening value. Powden’s review supports clinical utility across techniques, aligning with podiatric evidence-based standards.
In stroke rehab, post-Botox gains validate responsiveness. For podiatrists, it integrates into gait analysis, outperforming static measures for dynamic deficits.